

On Milk, Homogenization, and Lactase Deficiency
On Milk, Homogenization, and Lactase Deficiency

I want to preface this article by saying that I think milk is a very nutritious food and figuring out where your intolerance lies is important. It is equally important to be aware of its “level of digestibility” and use it as a gauge to inform yourself about your current state of health. This will be my humble attempt at presenting what I think modern milk is, why the rate of its “intolerance” is rising, and what a possible solution is.
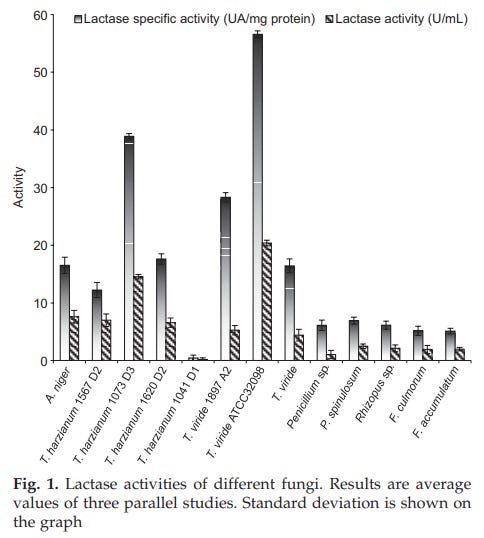
Milk in most supermarkets is fortified, pasteurized, and homogenized. The fortification of milk with vitamins A and D is mandated by the FDA, the reasoning being when milk is reduced from 3.25-4% (whole) to 1-2% (or skim), the lost fat-soluble vitamins should be replaced. The recent addition of whole vitamin D milk on supermarket shelves is a break in this pattern. Supplements of any kind carry with them the possibility of impurities, which tend to disrupt digestion and are quite allergenic. Fortified milk carries this risk. An additional point that must be made is in regards to the rise in “lactose-free” milk, which contains a plant/fungi-derived lactase enzyme used to break down the lactose into its sweeter monosaccharides (glucose and galactose). Lactase that is commercially produced is usually extracted from various molds like Aspergillus niger or Aspergillus oryzae (Seyis et al., 2004). These molds, amongst others, show a great deal of promise to lactase manufacturers. Unfortunately, the lactase enzymes that are added to milk are often contaminated with the molds themselves, acting as allergens.
A belief that has recently been revived in online health spheres is that the pasteurization of raw milk is the culprit behind people’s growing inability to digest milk, the detrimental effects of high heat destroying the enzymes, bacteria, and nutrients that aid in its digestion. I do not believe this to be the case, and a fairly strong argument can be made against it (the increased concentration of bacteria in raw milk can be allergenic and a source of endotoxin, repopulating an otherwise sterile small intestine with foreign bacteria). Whether the increasing number of news articles on the dangers of raw milk and the hospitalizations from its outbreaks are simply propaganda aimed at closing down family farms that produce raw milk, proceeding with caution with any food high in bacteria is wise. If raw milk fares well with you, it is far superior to commercial milk.
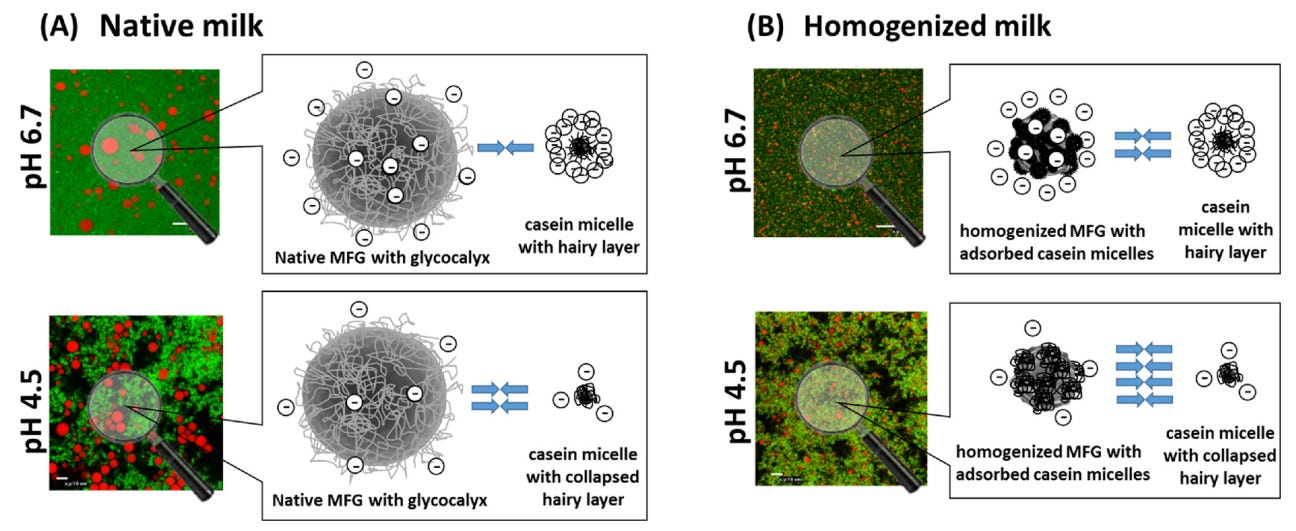
I think it is homogenization, not pasteurization, that makes commercial milk especially dangerous. Homogenization is the process of shrinking the fat globules in the milk by moving them through a fine strainer, causing the fat to shrink and incorporate with the rest of the milk. These liposomes are reduced from approximately 15 microns to 2. This is thought of as purely a cosmetic “procedure”, but on a second look is far from it.
In their natural state, the casein micelles (and other milk proteins) and the milk fat globules are negatively charged and relatively stable, and the electrostatic and steric repulsions prevent contact between them. Homogenization alters the surface properties of both, causing the casein micelles to adsorb into the fat globules (Obeid et al., 2019). Similar results have been experimentally demonstrated with xanthine oxidase and the bovine folate receptor, the latter being implicated in autism (Harrison, 2006).
The issues arise when these liposomes are persorbed through the lining of the intestine and into the bloodstream. Simply put, the fat globules act as a trojan horse for the milk proteins. It has been known for more than a century now that when undigested proteins/peptides end up in the bloodstream (as is the case with vaccines for example), they induce an immune response by increasing inflammation and the production of antibodies. I think drinking homogenized milk is a reasonable way of developing a casein allergy or facilitating the production of autoantibodies against the bovine folate receptor, blocking folate’s uptake by the brain. Children with autism seem to benefit from excluding commercial milk from their diet.
“In 1903 Arthus, in Lausanne, showed that a first intravenous injection of serum on a rabbit causes anaphylaxis, i.e. three weeks after the first injection the rabbit is hypersensitive to the second injection. The phenomenon of anaphylaxis was becoming of general application. Instead of applying only to toxins and toxalbumins, it held good for all proteins, whether toxic at the first injection or not.” - Charles Richet during his Nobel lecture in 1913
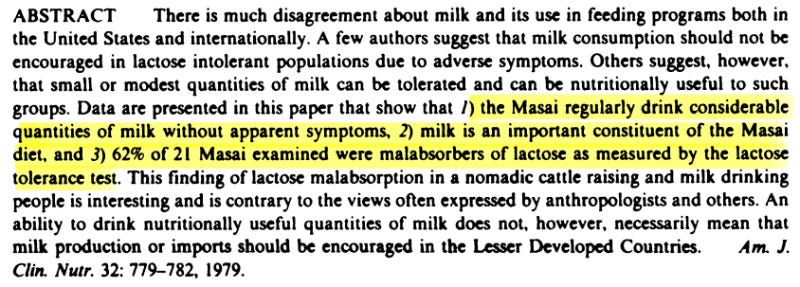
If the abovementioned are taken into account and milk intolerance still persists, then the focus should be directed at resolving SIBO or the existing lactase deficiency. Due to the abysmal state of health of the general public, small intestinal bacterial overgrowth is quite common. Ideally, the milk sugar lactose is digested in the small intestine with the help of the enzyme lactase and very little of it reaches the large intestine. In a state of low metabolism when the pH of stomach acid is dysregulated, reverse peristalsis during the night and times of stress can cause bacteria to repopulate the small intestine and ferment on the lactose, causing symptoms of what’s described by mainstream medicine as “lactose intolerance”. Keeping the small intestine free of bacteria with the help of insoluble fiber (carrot salad), safe antibiotics, cascara, and a low-starch diet can help. It is important to keep in mind that a lactase deficiency can still persist despite the small intestine being sterile. The Masai children of East Africa whose diet consists mainly of milk still experience symptoms of lactose malabsorption, despite their continued exposure to lactose in raw milk (Jackson et al., 1979). With more exposure, bacteria in the intestines adapt and produce less hydrogen gas (Forsgard, 2019).
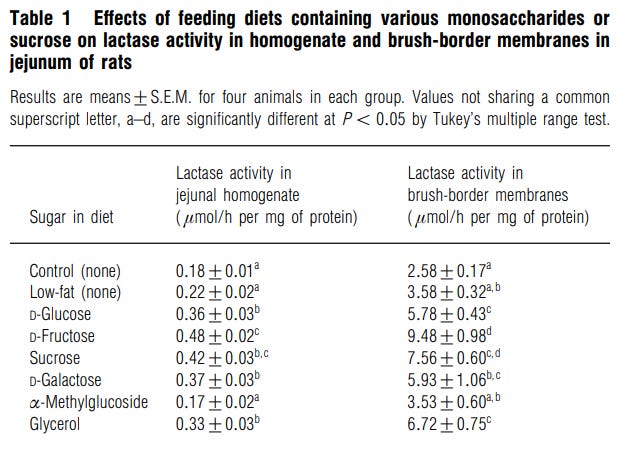
Research on ways to increase lactase production in the small intestine is scarce since its lack of production is ascribed to the natural aging cycle within genes. In rats, lactase activity and its mRNA levels are increased by the consumption of various carbohydrates, with fructose causing the biggest increase followed by sucrose (Tanaka et al., 1998). Adding ordinary table sugar to milk can aid in the digestion of lactose.
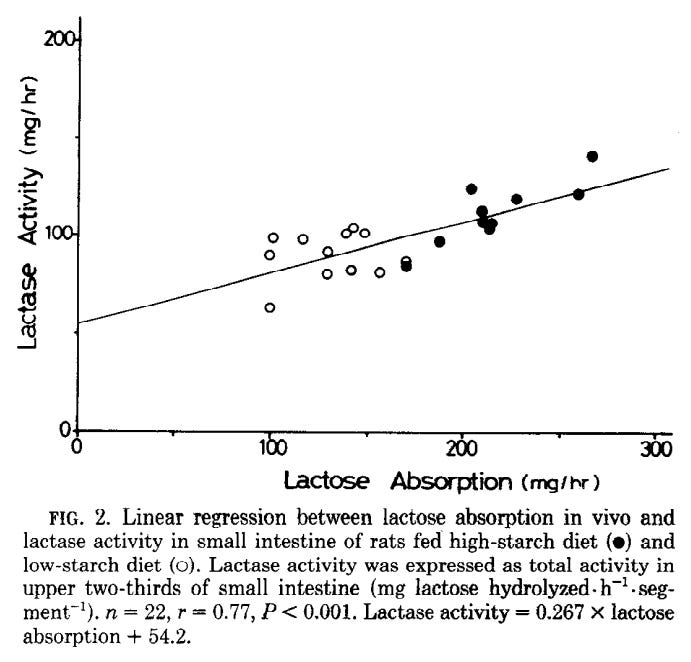
An increase in lactase activity is also observed in rats fed a high-starch diet, so I think it is reasonable to assume that a diet devoid of carbohydrates (keto, carnivore, etc.) can lower lactase activity in the small intestine and cause lactose intolerance (Leichter et al., 1984).
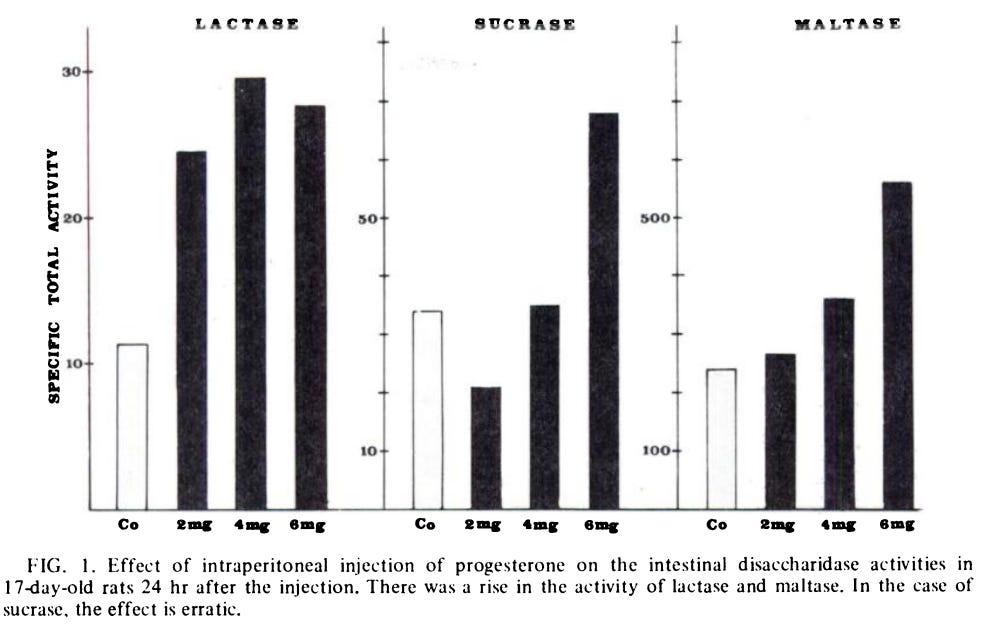
A single injection of progesterone increases the activity of various brush broader enzymes, including lactase. Additionally, there was a synergistic effect on lactose activity when progesterone was administered together with goat milk (Goldstein et al., 1974).
I think the overarching idea between these studies is that increasing the metabolic rate will allow the body to produce the lactase enzyme, and healing the small intestine will prevent the loss of the enzyme. The knee-jerk prescription of the inability to digest lactose to an arbitrary set of genes is simply a cop-out by a medical establishment that is unfortunately too ignorant and incompetent to see the bigger picture.
References
Seyis, Isil & Aksoz, Nilufer. (2004). Production of Lactase by Trichoderma sp. Food Technology and Biotechnology. 42.
Obeid, S., Guyomarc’h, F., Francius, G., Guillemin, H., Wu, X., Pezennec, S., … Lopez, C. (2019). The surface properties of milk fat globules govern their interactions with the caseins: Role of homogenization and pH probed by AFM force spectroscopy. Colloids and Surfaces B: Biointerfaces, 182, 110363. doi:10.1016/j.colsurfb.2019.11036
Harrison, R. (2006). Milk xanthine oxidase: Properties and physiological roles. International Dairy Journal, 16(6), 546–554. doi:10.1016/j.idairyj.2005.08.016
Jackson, R. T., & Latham, M. C. (1979). Lactose malabsorption among Masai children of East Africa. The American Journal of Clinical Nutrition, 32(4), 779–782. doi:10.1093/ajcn/32.4.779
Forsgard R. (2019). Lactose digestion in humans: intestinal lactase appears to be constitutive whereas the colonic microbiome is adaptable. The American Journal of Clinical Nutrition, doi:10.1093/ajcn/nqz104
Tanaka, T., Kishi, K., Igawa, M., Takase, S., & Goda, T. (1998). Dietary carbohydrates enhance lactase/phlorizin hydrolase gene expression at a transcription level in rat jejunum. Biochemical Journal, 331(1), 225–230. doi:10.1042/bj3310225
Leichter, J., Goda, T., Bhandari, S. D., Bustamante, S., & Koldovsky, O. (1984). Relation between dietary-induced increase of intestinal lactase activity and lactose digestion and absorption in adult rats. American Journal of Physiology-Gastrointestinal and Liver Physiology, 247(6), G729–G735. doi:10.1152/ajpgi.1984.247.6.g729
Goldstein, R., Landau, H., & Freier, S. (1974). Disaccharidase activities in the rat intestine. II. Effect of progesterone. The American Journal of Clinical Nutrition, 27(8), 845–849. doi:10.1093/ajcn/27.8.845
I wonder if there is a relationship between the amount of milk fat and sufficiency of lactose. Many years ago I discovered that I could digest 1%, 2% and full-fat milk just fine but could not digest skim milk - it gave me cramps and diarrhea.
excellent work