

Hypoglycemia, PMS, and Metabolism as Legal Defense.
Hypoglycemia, PMS, and Metabolism as Legal Defense.
"Your Honor, my client has the metabolic rate of a juvenile. He can't be tried as an adult."

The idea that the mentally insane are treated differently in a court of law compared to the general “healthy” public isn’t anything new. If the psychiatric evaluation designates a criminal as insane, the punishment is often relatively light. The question then arises is what constitutes insanity, or rather can it be linked to a physiological state so that its parameters are more concrete. Georgi mentioned in one of his articles that numerous studies nowadays have started to acknowledge the metabolic origin of all psychiatric disorders, admitting that proper energy metabolism governs the processes of a healthy mind.
In his book “It’s Not Your Mind, It’s Your Liver”, Broda made this case decades ago. He saw that hypoglycemia brought on by poor liver health (which is in turn a symptom of low thyroid function) gave rise to several mental symptoms, hence the title of the book. Dread, feelings of doom and uncertainty, aggression, fear, etc can all be reliably linked to poor sugar metabolism, but typically, hypoglycemia is rarely focused on as a cause. Broda made the case that hypoglycemia can be classified as transient insanity because of the acute change in behavior and attitude that takes place in something like diabetes. When starved of glucose, the brain tends to sway towards the “not responsible for my actions” orientation. Among arsonists, nearly half were found to be hypoglycemic (Virkkunen, 1984). It is important to note that alcohol is a known “hypoglycemic agent”; most violent drunks would benefit from frequent snacking. A very similar response takes place in hypoglycemic children during their night terrors (which happens during the day as well).
“The child is found sitting up in bed, or crouching in a corner with hands outstretched, as if to shield himself. Sometimes he is trying to get out of the room, or to open the door; or he will escape from the room and run screaming down the staircase: His face expresses the wildest alarm, his eyes are opened, with pupils dilated, and he gazes intensively widely in the direction of the apparition. The period of terror lasts a few to thirty minutes. The child presently recognizes his surroundings, but he sweats and trembles, turns pale, looks shocked and exhausted.” (Patrick, 1964)
I’ll often hear the argument that this sounds overly reductionist, that linking such a seemingly complex set of psychological symptoms to a few biochemical processes is too simplistic. If prescribing these emotions or mental symptoms to something intangible, abstract, or metaphysical makes coping easier, then by all means. I don’t think this takes away from the boundless wonder and mystery that is already around us, much of which we cannot explain through “scientific vigor”. The paranormal, synchronicities, and apparitions aren’t single-caused and our understanding of them should be expansive.
Interestingly, hypoglycemia as a legal defense has successfully been used before. A diabetic man was caught shoplifting, and he argued that his behavior was brought on by confusion from his insulin shot. The case was dismissed (Toth, 1990).
A legal firm collected a literature review on the psychological effects of hypoglycemia as part of a defense for their diabetic client who was charged with vehicular homicide, and they concluded that hypoglycemia can act as a “mitigating factor in litigation” (Piotrowski, 1997).
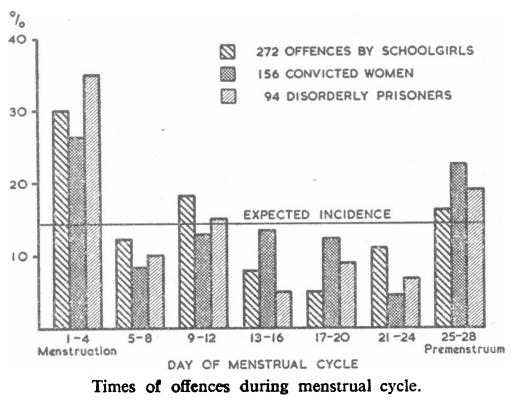
Katharina Dalton is popularly known for her work with “progesterone babies”, when she found that women who supplemented progesterone in treating their PMS had babies with superior intelligence. One of the less discussed aspects of her work surrounds the idea of crime and menstruation. In one of her studies in a women’s prison, Dalton found that nearly half committed their crime during menstruation, or a few days prior (Dalton, 1961).
After drawing the successful connection between high estrogen, premenstrual syndrome, psychiatric disturbances, and crime, she acted as a witness in defense of several women in court!
Case #1: She had twenty-six convictions; criminal damage, theft, trespassing, writing threatening letters, possessing a dangerous weapon, and a fatal stabbing. While in detention she attempted arson, escape, hanging, strangling, drowning, smashed windows, and cut her wrists.
Case #2: She attempted suicide at the age of 14, swallowed weedkiller, ran away from home, shaved her head and eyebrows, cut her face, abused alcohol, set fire to her home, attempted arson, cut her wrists, and tried to strangle herself.
Case #3: She made false 911 calls, did criminal damage, assaulted three policewomen, attempted to hang herself, threatened to kill her grandmother, slashed her wrists, and threw a knife at a man.
All of the abovementioned women successfully pleaded diminished responsibility and were started on progesterone treatment (Dalton, 1980). In the ‘80s, these cases became a source of controversy amongst prosecutors, attorneys, doctors, and feminists in Britain. The Canadian courts also explored the subject, but refused to accept PMS “as a substantive defense to criminal charges”. They did, however, consider it as a “mitigating factor” in several cases (Meehan et al., 1986). Katharina herself was careful to note that this defense could be very easily abused.
“Those few women who lose control of themselves for a day or two, month after month, need help and help is available. However, they must not be confused with the other 99.9 percent of women who are well able to control their actions. PMS is not a universal defense, nor should it be allowed to become one. Medical evidence is required by the court and the doctor must become fully conversant with the recognition, diagnosis, and treatment of the syndrome…We must remain suspicious of women who plead that premenstrual syndrome is a reason for mitigation or diminished responsibility; good diagnostic proof is still necessary. This study shows another aspect of premenstrual syndrome and the necessity for the general practitioner to be able to diagnose and treat this condition. The cost of keeping one woman in prison is 105.00 pounds per week. The cost of progesterone treatment is a mere fraction of that sum.“ - Katharina Dalton
I often joke about the idea of metabolism being interwoven with the criminal courts and find it quite amusing how broad the range of possibilities and outcomes it’d produce, imagining one day defense lawyers arguing that their adult clients should be tried as juveniles because their metabolism is that of a teenager (isn’t that what really matters?). The flip side of that coin, which is the more realistic option and the one I’ve presented here, is being granted a lighter sentence on the account of having an impaired metabolism (where it truly applies), a “temporary episode of insanity or true confusion”. This isn’t an argument to relieve individuals from autonomy because even in the worst of conditions, people have shown that abandoning morality is a matter of choice, not an automatic process governed by substances and hormones. Solzhenitsyn talked about how the priests were usually the last ones to lose their minds in the camps, and how the Soviet astrophysicist Kozyrev (the man who Ray has mentioned so much) was only able to stay sane in the gulags (compared to those around him) by:
“thinking of the eternal and infinite: of the order of the Universe - and of its Supreme Spirit; of the stars; of their internal state; and what Time and the passing of Time really are.”
This is merely a thought experiment about the degree to which our metabolic rate affects our decision-making, and to what extent it can cause us to abandon our principles when confronted with degrees of environmental stress. I find that I am far more kinder, understanding, quicker to action, and less likely to sin when I’m burning warmer. These are realities of our biology that we must acknowledge if there is going to be any meaningful discourse about the influence of culture, religion, and biology on each other.
References
Dalton, K. (1961). Menstruation and Crime. BMJ, 2(5269), 1752–1753. doi:10.1136/bmj.2.5269.1752
Dalton, K. (1980). Cyclical Criminal Acts in Premenstrual Syndrome. The Lancet, 316(8203), 1070–1071. doi:10.1016/s0140-6736(80)92286-2
Meehan E, MacRae K. Legal implications of premenstrual syndrome: a Canadian perspective. CMAJ. 1986 Sep 15;135(6):601-8. PMID: 3756691; PMCID: PMC1491301.
Patrick, A. (1964). SOME ASPECTS OF HYPOGLYCÆMIA. The Lancet, 284(7371), 1230–1233. doi:10.1016/s0140-6736(64)91062-1
Piotrowski, C. (1997). Hypoglycemia as a Mitigating Factor in Vehicular Accidents. Perceptual and Motor Skills, 84(3_suppl), 1241–1242. doi:10.2466/pms.1997.84.3c.1241
Toth, E. L. (1990). Brain Wave on the Witness Stand. Diabetes Care, 13(7), 817–818. doi:10.2337/diacare.13.7.817
Virkkunen, M. (1984). Reactive hypoglycemic tendency among arsonists. Acta Psychiatrica Scandinavica, 69(5), 445–452. doi:10.1111/j.1600-0447.1984.tb02517.x