

Homosexuality as a Symptom of Metabolic Disorder: War, Prolactin, and Course Correction.
Homosexuality as a Symptom of Metabolic Disorder: War, Prolactin, and Course Correction.

In the previous article “How to Sire More Sons or Daughters”, I discussed the relationship between environmental stress and the sex ratio at birth; stress decreases the likelihood of male births. This has resulted in a slowly developing trend of fewer births of boys in industrialized nations. Sexual preference and attraction are also largely dependent on an organism’s metabolism and this article will touch upon some of the factors involved. Because of the controversial nature of this topic, you will find studies providing evidence to the contrary of what’s presented here, and so it’s ultimately up to you to form your own opinion. It’d be asinine for me to present the current cultural beliefs about homosexuality (and other deviations) because of the ever-increasing fluidity and generality of its definitions and prescribed causes. If it’s of a genetic origin, how does it explain the sharp increase in the incidence of these sexual orientations over the past decade alone? How does a genetic trait pass itself down when reproduction for the ingroup is a physical impossibility? If nurture is largely to blame for the increase, then “conversion therapy” which has so extensively been vilified is alive and actively promoted.
What first drew my attention to this topic was a study I had accidentally come across that found a positive correlation between prenatal stress and the rate of male homosexuality after the Second World War in six districts in Germany (Dörner et al., 1980). The author, Günter Dörner, was a German neuroendocrinologist who when asked in a brief biography which among his discoveries or concepts he finds most interesting and valuable, replied:
“I would like to point out the discovery that intercellular messengers, such as hormones, neurotransmitters, and cytokines, are environment and gene-dependent organizers of the brain as controllers of the neuro-endocrine-immune system (NEIS). Thus, unphysiological concentrations of neurotransmitters, hormones, and cytokines can act during critical organization periods of the NEIS as “endogenous teratogens”, leading to pre- and early postnatally acquired, life-long malfunctions and important diseases of reproduction, metabolism, and the cardiovascular system, of benign and malignant growth, of information processing and of the immune system.“
I mention this because it is important to note that his working framework is essentially that of the “bioenergetic” or the “treatment of the organism as an inseparable part of its environment” view of life. He goes on to say:
“When the mother represents the immediate environment of the unborn and newborn – the following burden by the environment should be prohibited or timely corrected, respectively: Iodine deficiency, gestational diabetes, oxygen deficiency, stress, gestoses, infections, and vitamin deficiencies, quantitative and/or qualitative malnutrition, ionizing radiation, and most of all, environmental chemicals which act as “neuroendocrine disruptors” and “neuro-endocrine-immune teratogens”, alcohol, nicotine, drugs, psychosocial deprivation, and abnormal concentrations of hormones and neurotransmitters.” (Dörner, 2008)
Anyhow, Dörner interviewed 100 heterosexual and 100 bi/homosexual men about the maternal stressful events that took place during their prenatal life. 73% of the stressful events reported were caused by influences of war (bombardment, death of a father, etc.), or unwanted pregnancies. The table below shows the significantly increased incidence of prenatal stress in bisexual and homosexual men (Dörner et al, 1983).

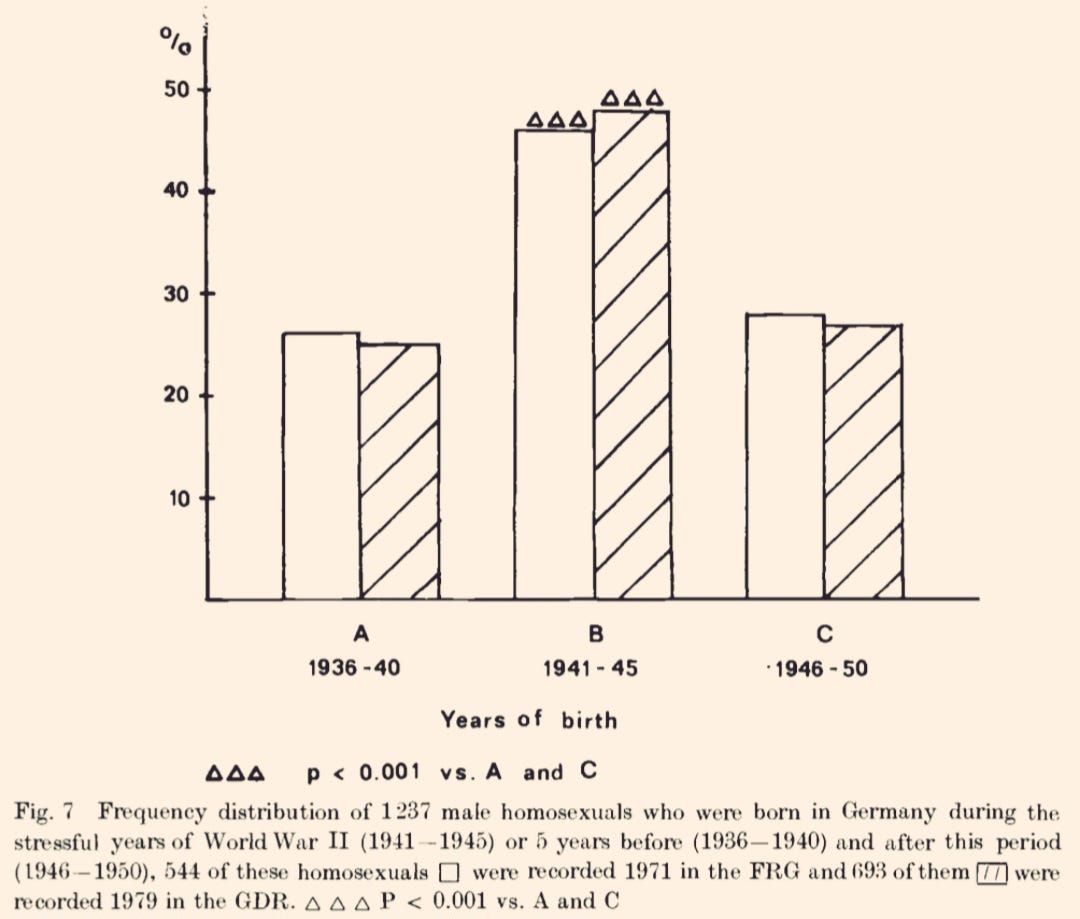
Similar results were found by a different group of German scientists, who studied 1237 male homosexuals before, during, and after the Second World War and found that close to 50% of their subjects were born during the stressful years (1941-1945) (Dannecker et al., 1974).
Through a series of experiments, Dörner demonstrated that in an androgen deficiency, the male fetus develops a female-differentiated brain in the “sex-specific hypothalamic differentiation” phase which is then activated during the postpubertal “sex nonspecific hypothalamic organization” phase by the surge of androgens. This may explain why some experiments have found no difference between serum androgen levels of homo/heterosexual individuals. In one of his experiments (as well as experiments before him conducted on rats), injecting even a single dose of estrogen caused a positive feedback loop to form in homosexual subjects compared to heterosexuals, supporting his hypothesis about the difference in brain differentiation. (Dörner et al, 1975).
“As an increased amount of estradiol is released from the ovaries during the first half of the menstrual-estrus cycle, eventually an LH surge is triggered by the hypothalamic-pituitary network. This surge inhibits further estradiol production and induces ovulation and increased progesterone release, which, in turn, eventually causes estradiol production to also gradually rise, and thus the cycle starts over again. The entire process can be manipulated in most females merely by injecting high levels of estradiol. In the male, however, the hypothalamic-pituitary network is usually organized in such a way as to prevent major estradiol-induced LH surges.“

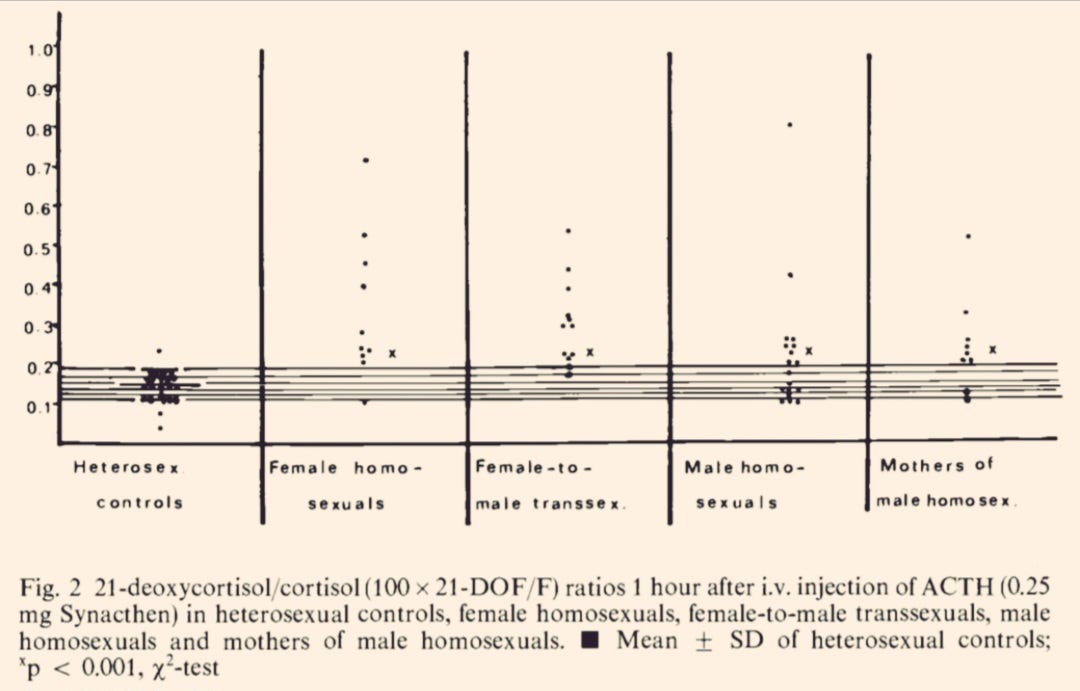
A marked difference in endocrine response to a hormone injection between homo/trans/heterosexuals was also demonstrated in a different study. When injected with the pituitary hormone, ACTH, there was an abnormal ratio of adrenal hormone production in female homo/transsexuals with what the authors concluded was the result of a 21 hydroxylase deficiency. Congenital adrenal hyperplasia (CAH), which is diagnosed with a 21 hydroxylase deficiency, leads to salt wasting, hirsutism, and virilization as there is an increased production of adrenal androgens and stress hormones. Meaning, that an enzyme deficiency that is present at birth, causes an overproduction of adrenal androgens in women, effectively aiding in the development of a male-differentiated brain. They are more likely to prefer traditionally masculine hobbies, and sports, and have fewer fantasies about romance or marriage. They also tend to be more attracted to their sex (Ellis et al., 1987).
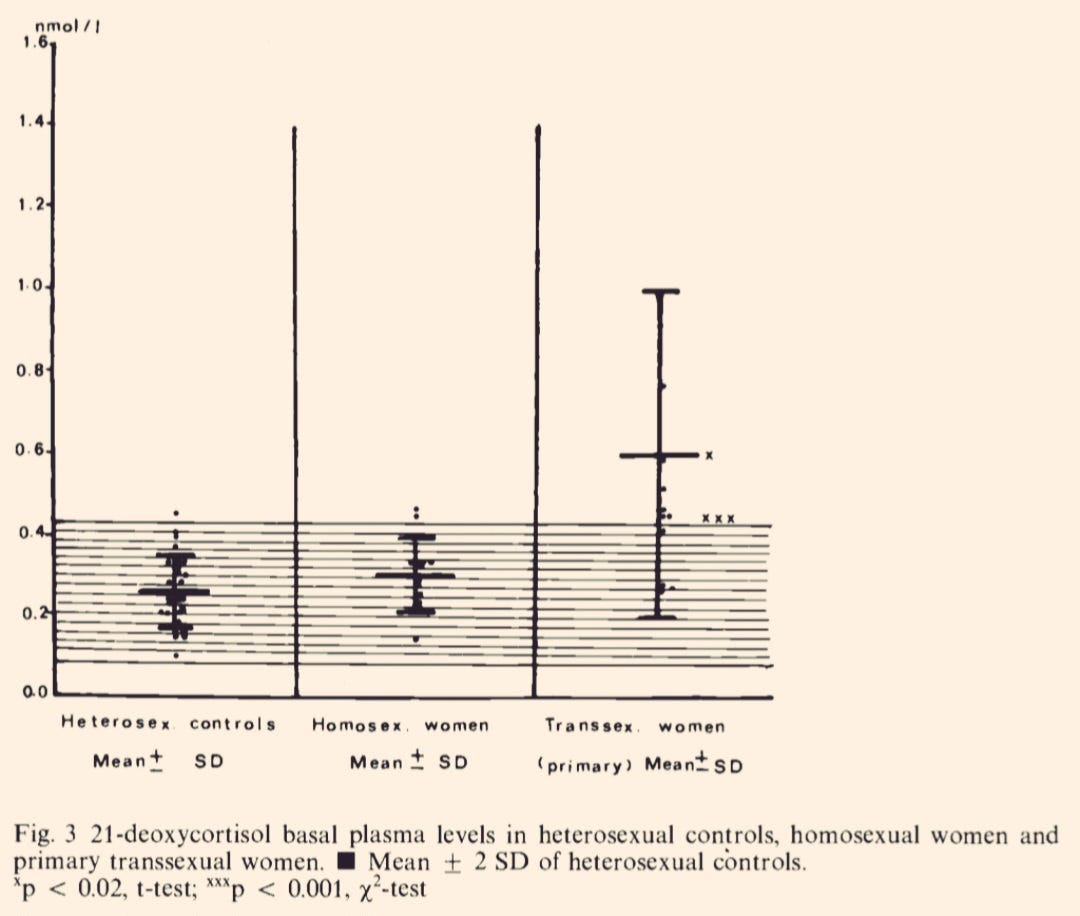
At rest, transsexual women showed higher baseline cortisol levels than homo/heterosexual women. (Dörner et al., 1991).
As a general rule, less energy is expanded and more is conserved during stress as estrogen, prolactin, serotonin, and cortisol lower oxygen consumption and slow cellular processes. Hyperprolactinemia, for example, has been implicated in swaying the psycho-sexual orientation in male subjects towards homosexuality, partly by opposing and lowering brain androgen levels in pre and post-natal life. There is an interesting paper by Roper, called “The Etiology of Male Homosexuality” where a hypothesis is put forth about stress-induced hyperprolactinemia predisposing the brain of the male infant to homosexual tendencies in adulthood (Roper, 1996). What I find especially comical, however, is the conclusion of the author where instead of viewing it as a pathology, it is labeled a simple “biological variation”. How can a stress-induced rise in a hormone that is implicated in several degenerative diseases give rise to a neutral “variation”? Interestingly enough, one of the most effective dopamine agonists, and prolactin/serotonin antagonists, lisuride, has been used to reverse same-sex behavior in male rats (Götz et al., 1991, Tönjes et al., 1989). Both estrogen and melatonin increase prolactin production, so keeping exposure to darkness low and abstaining from supplementing with melatonin can be helpful. As a quick tangent, a recent study found 22/25 melatonin gummy brands to contain upwards of 3.5 times more of the hormone than advertised, keeping in mind the fact that melatonin has been shown to shrink the gonads (possibly through increasing prolactin production). Bromocriptine is another safe and effective prolactin antagonist and dopamine agonist.
One of the more frequently talked about points lately has been about the influence of estrogen and progesterone on the experience of the “fullness” of an orgasm; where the inhibition of the latter balances the excitation of the former. In a progesterone or vitamin E deficiency, orgasm is usually described as unfulfilling.
“Having an orgasm without enough vitamin E would be like sneezing without first inhaling, the effect is a series of very small, quick sneezes.“ - Ray Peat
It is this estrogen-driven “unresolved” state that I think partly drives increasingly bizarre novelty-seeking sexual behaviors: compounding sets of stimulations that never fully conclude.
One of my favorite anecdotes of what would now be classified as “conversion therapy” is two case studies of teenagers, who had been admitted to a psychiatric clinic with various cognitive disorders, anti-social behaviors, and homosexual tendencies. Treatment with dehydroepiandrosterone (DHEA), one of the youth-associated hormones that converts downstream to the more potent androgens, quickly corrected them (Sands et al., 1952). A brief excerpt is below.


There are many more points that I did not get to address in this article simply because of how dense this topic is, but it is clear in my opinion that when people refer to homosexuality as “genetically acquired”, what they really mean is nurture driven by the intrauterine conditions that have shaped the developing brain during pre and even postnatal life. Cultural forces do exert their influence on thought/temperament/personality (as well as biology), but the receptivity or the orientation of the pre/postnatal brain (mediated by androgens, sex and stress hormones, neurotransmitters, etc) is what these forces must first interact and tug with. When, for example, people admit that they’ve always (since childhood) felt an attraction towards the same sex, I don’t think they are lying. There are reasons for feeling things, but the manner in which this culture jumps to conclusions and enacts policies to “affirm” them as indisputable and absolute truths, or even as a part of sound health, I find this, simply put, evil. To ascribe sexual orientation or gender to only an arbitrary set of genes is to ignore the mountain of evidence demonstrating the different AND evolving hormonal profiles between homosexual and heterosexual individuals.
It is far harder to fix a broken man than to raise a healthy child, but we’re not as static or time-stuck as we’d like to think and the extent of our ability to regenerate or course correct is still a mystery.
References
Dannecker, M.; Reiche, R.: Der gewöhnliche Homosexuelle. Eine soziologische Untersuchungüber männliche Homosexuelle in der Bundesrepublik. Frankfurt/Main: S. Fischer-Verlag 1974, S. 201.
Dörner G, Geier T, Ahrens L, et al. Prenatal stress as possible aetiogenetic factor of homosexuality in human males. Endokrinologie. 1980 Jun;75(3):365-368. PMID: 7428712.
Dörner, G.; Schenk, B.; Schmiedel, B.; Ahrens, L. (1983). Stressful Events in Prenatal Life of Bi- and Homosexual Men. Experimental and Clinical Endocrinology & Diabetes, 81(1), 83–87. doi:10.1055/s-0029-1210210
Dörner, G., Rohde, W., Stahl, F., Krell, L., & Masius, W.-G. (1975). A neuroendocrine predisposition for homosexuality in men. Archives of Sexual Behavior, 4(1), 1–8. doi:10.1007/bf01541882
Dörner, G. (2008). Günter Dörner, neuroendocrinologist. Human_ontogenetics, 2(1), 5–9. doi:10.1002/huon.200800004
Dörner, G., Poppe, I., Stahl, F., Kölzsch, J., & Uebelhack, R. (1991). Gene- and Environment-Dependent Neuroendocrine Etiogenesis of Homosexuality and Transsexualism. Experimental and Clinical Endocrinology & Diabetes, 98(05), 141–150. doi:10.1055/s-0029-1211110
Ellis, L., & Ames, M. A. (1987). Neurohormonal functioning and sexual orientation: A theory of homosexuality–heterosexuality. Psychological Bulletin, 101(2), 233–258. doi:10.1037/0033-2909.101.2.233
Götz, F., Tönjes, R., Maywald, J., & Dörner, G. (1991). Short- and Long-term Effects of a Dopamine Agonist (Lisuride) on Sex-specific Behavioural Patterns in Rats. Experimental and Clinical Endocrinology & Diabetes, 98(05), 111–121. doi:10.1055/s-0029-1211107
Roper, W. G. (1996). The etiology of male homosexuality. Medical Hypotheses, 46(2), 85–88. doi:10.1016/s0306-9877(96)90006-7
Sands, D. E., & Chamberlain, G. H. A. (1952). Treatment of Inadequate Personality in Juveniles by Dehydroisoandrosterone. BMJ, 2(4775), 66–68. doi:10.1136/bmj.2.4775.66
Tönjes, R., Götz, F., Maywald, J., & Dörner, G. (1989). Influence of a Dopamine Agonist (Lisuride) on Sex-Specific Behavioural Patterns in Rats. II. Long-Term Effects*). Experimental and Clinical Endocrinology & Diabetes, 94(04/05), 48–54. doi:10.1055/s-0029-1210879
Fascinating. Thank you for taking the time to do the research, as always. I have a question. If, hypothetically, one wanted to limit the chances of such adaptation in their own offspring, what would you say would be reliable metrics (temperature aside) to keep an eye on during pregnancy?
This is maybe a bit of a pie in the sky, but do you think that to minimise stress one could try to optimise the intake of electrolytes and B vitamins - and “the rest will follow” ?